Part 3: All About The Vaccine
mRNA, adenoviral vector as well as inactivated whole-virus vaccines are now in widespread use, and a subunit vaccine is in a final stage of authorization. They all rely on the native viral spike protein (S) of SARS-CoV-2 for inducing potently neutralizing antibodies, but the presentation of this key antigen to the immune system differs substantially between the different categories of vaccines.
In this part we will explore the way the vaccine presents the spike protein, lipid nano-particles, as well as a review on how the public policy of using a spike protein based vaccine during an active SARS pandemic evolved.
Antibody Targets
The potency of antibodies depends on high-affinity interactions with specific parts of the complex three-dimensional structure of the spike in a native conformation.
B-cell humoral immunity is the target for “long-term” immunity for any pathogen. Efficient formation of such antibodies by B cells requires helper functions of CD4 T cells that are specifically stimulated by peptides derived from the same antigen in complex with MHCII molecules (innate immune system).
Other components of cellular immunity, such as CD8 T cells, also contribute to immune responses after SARS-CoV-2 infection or vaccination, although their role in COVID-19 infections and protection from disease is still incompletely resolved.
It is a significant note to cite the role of CD8+ T-cells as being “incompletely resolved”. Government agencies have been using “Waning immunity” as the epidemiological purpose of requiring booster shots. This recommendation is being forwarded from the foundation of the loss of CD8+ T-cell concentration in the blood. From part 2, we learned consistent exposure to an antigen may prime the immune system for ADE. With that knowledge, as well as the scientific admission that B-cell immunity is preferred, what reason can a pharmaceutical regulator allow for policy to be based on CD8+ T-cell concentration?
Vaccine Types
Irrespective of vaccine type, all have to cope with the intrinsic problem of conformational instability of the spike protein, whether it is synthesized in the vaccinee after genetic vaccination or in cell culture systems for production of conventional vaccines.
The first category type is mRNA and the second are adenoviral vector vaccines, both of which do not contain the spike protein but provide genetic information for its biosynthesis in body cells of the vaccinee.
mRNA and N1-methylpseudouridine-m1Ψ
RNA vaccines contain fully functional mRNAs that can be translated directly into the S protein. Additional biosynthetic steps are required with adenovirus vector vaccines, including intranuclear transcription of the vector DNA into RNA and processing to generate functional mRNAs. It is believed that muscle cells, fibroblasts, endothelial cells, and/or immune cells such as dendritic cells contribute to the expression of S after intramuscular vaccination
ER—endoplasmic reticulum; ERGIC—endoplasmic reticulum Golgi intermediate compartment; TGN—Trans Golgi Network; RNP—Ribonucleoprotein; Viral proteins: S—spike, M—membrane; E—envelope; N—nucleoprotein.
BioNTech-Pfizer and Moderna contain codon-optimized sequences for efficient expression of the full-length S protein and use the authentic signal sequence for its biosynthesis. Both constructs include the two stabilizing mutations in S2 (K986P and V987P).
https://www.nature.com/articles/s41541-021-00369-6#Fig3
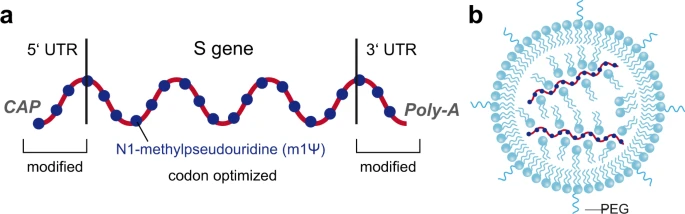
Both mRNA vaccines have modulated 5′ and 3′ untranslated sequences to optimize mRNA stability and translation efficiency, and all uridines are replaced by N1-methylpseudouridine (m1Ψ) to further increase RNA stability and to reduce innate immune responses.
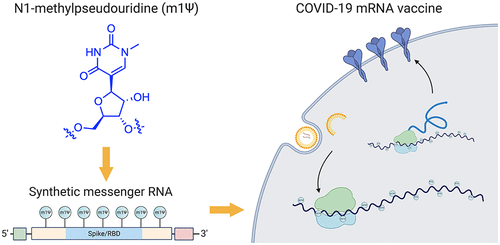

Non-natural RNA nucleobase N1-methylpseudouridine (m1Ψ); enhances immune evasion and protein production.
- A 5′-cap (m7(3′OMeG)(5′)ppp(5′)(2′OMeA)pG, commonly referred to as trinucleotide “cap 1”) that helps recruit the ribosome and protect the RNA from degradation.
- A 5′-untranslated region (UTR) derived from the human α-globin mRNA with an optimized Kozak sequence that helps drive high levels of translation from the correct start codon.
- A codon-optimized coding sequence that specifies production of the transmembrane-anchored immunogenic SARS-CoV-2 spike glycoprotein.
- A 3′-UTR consisting of two sequences derived from the amino-terminal enhancer of split mRNA and the mitochondrial encoded 12S rRNA, which aids high levels of protein expression by stabilizing the RNA.
- An unusual 3′-terminus consisting of two segmented poly(adenosine) tracts. The poly(adenosine) stretches increase mRNA stability, while the segmented structure helps reduce unwanted recombination during plasmid production.
It is important to note that in many studies, the specific contributions of each of these mechanisms to mRNA immunogenicity have not been explicitly defined. In such cases, an mRNA modification may be exerting its activity by altering antisense transcript synthesis, mRNA structure, immune recognition, or some combination thereof.
Incorporation of m1Ψ increases the size and abundance of polysomes, leading them to propose that the more rapid translation initiation and slower elongation of m1Ψ mRNAs may coordinately increase their half-life as well as induce productive interactions with the ribosome.
Further studies provided support for a model in which secondary structure in the coding sequence, which can be enforced by m1Ψ, may increase mRNA functional half-life independent of codon optimality.
While the modular nature of mRNA vaccines has led to considerable enthusiasm, the combinatorial space of elements that contribute to their activity (including caps, coding sequence, codons, UTRs, and modifications) is massive in scale, and relatively few RNA modifications have been comparatively evaluated in a systematic manner.
https://pubs.acs.org/doi/10.1021/acscentsci.1c00197
Adenovirus Vector Vaccines
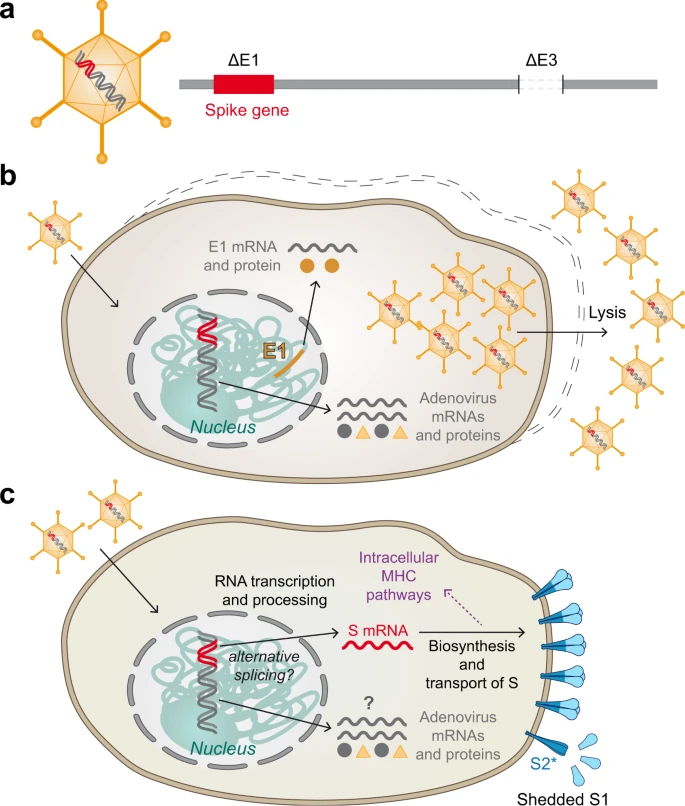
Compared to mRNA vaccines, adenovirus-vector vaccines comprise several additional layers of complexity (including production in mammalian cell cultures) that can lead to heterogeneities of immune reactions and adverse effects. Variations include (but are not limited to) the type of adenovirus used as a vector (Janssen-Johnson&Johnson—human adenovirus #26), genetic modifications of the vector, the cell lines used for vaccine production, procedures for purification, and the specific design of the gene for expressing S.
The current adenovirus-vaccine vectors are the replacement of one of the early adenoviral genes (E1) for the full-length SARS-Cov-2 S gene in the adenoviral DNA and the additional deletion of E3. Production cell lines are derived from human embryonic retinal cells (PER.C6) for the Janssen vaccine.
Although in vitro model studies with one of the current adenovirus vector vaccines (ChAdOx1 nCoV-19) have shown that S-coding transcripts dominate the transcription patterns, rare aberrant splicing or polyadenylation site usage were observed. Alternative splice events might lead to the formation of C-terminally truncated and therefore soluble S protein. Such secreted forms may bind to ACE2-expressing endothelial cells and could contribute to thrombotic events via ADE mechanism. Janssen vaccine contains the two prolines in S2 but and mutated the S1/S2 furin cleavage site from 682-RRAS-685 to SRAG to avoid conversion of S into the post-fusion structure. https://www.nature.com/articles/s41541-021-00369-6#Tab1
mRNA in Liver converting to DNA
Preclinical studies of COVID-19 mRNA vaccine BNT162b2, developed by Pfizer and BioNTech, showed reversible hepatic effects in animals that received the BNT162b2 injection. Furthermore, a recent study showed that SARS-CoV-2 RNA can be reverse-transcribed and integrated into the genome of human cells.
The safety profile of BNT162b2 is currently only available from short-term clinical studies. Less common adverse effects of BNT162b2 have been reported, including pericarditis, arrhythmia, deep-vein thrombosis, pulmonary embolism, myocardial infarction, intracranial hemorrhage, and thrombocytopenia.
In pharmacokinetics data provided by Pfizer to European Medicines Agency (EMA), BNT162b2 biodistribution was studied in mice and rats by intra-muscular injection with radiolabeled LNP and luciferase modRNA. Radioactivity was detected in most tissues from the first time point (0.25 h), and results showed that the injection site and the liver were the major sites of distribution, with maximum concentrations observed at 8–48 h post-dose
Intracellular accumulation of LNP in hepatocytes (liver cells) has been demonstrated in vivo. A preclinical study on BNT162b2 showed that BNT162b2 enters the human cell line HEK293T (kidney) cells and leads to robust expression of BNT162b2 antigen.
A previous study on mRNA vaccines against H10N8 and H7N9 influenza viruses using a similar LNP delivery system showed that the mRNA vaccine can distribute rather nonspecifically to several organs such as liver, spleen, heart, kidney, lung, and brain, and the concentration in the liver is roughly 100 times lower than that of the intra-muscular injection site. In the assessment report on BNT162b2 provided to EMA by Pfizer, the pharmacokinetic distribution studies in rats demonstrated that a relatively large proportion (up to 18%) of the total dose distributes to the liver.
Liver cells also present the vaccine-derived SARS-CoV-2 spike protein, which could potentially make the liver cells targets for previously primed spike protein reactive cytotoxic T cells. There have been case reports on individuals who developed autoimmune hepatitis after BNT162b2 vaccination.
BNT162b2 can be reverse transcribed to DNA in liver cell line Huh7, and this may give rise to the concern if BNT162b2-derived DNA may be integrated into the host genome and affect the integrity of genomic DNA, which may potentially mediate genotoxic side effects. At this stage, we do not know if DNA reverse transcribed from BNT162b2 is integrated into the cell genome. Further studies are needed to demonstrate the effect of BNT162b2 on genomic integrity, including whole genome sequencing of cells exposed to BNT162b2, as well as tissues from human subjects who received BNT162b2 vaccination.
Human autonomous retrotransposon LINE-1 (long interspersed nuclear element-1) is a cellular endogenous reverse transcriptase and the only remaining active transposon in humans, able to retrotranspose itself and other nonautonomous elements, and ~17% of the human genome are comprised of LINE-1 sequences. A recent study showed that endogenous LINE-1 mediates reverse transcription and integration of SARS-CoV-2 sequences in the genomes of infected human cells. Furthermore, expression of endogenous LINE-1 is often increased upon viral infection, including SARS-CoV-2 infection.
Previous studies showed that LINE-1 retrotransposition activity is regulated by RNA metabolism, DNA damage response, and autophagy. Efficient retrotransposition of LINE-1 is often associated with cell cycle and nuclear envelope breakdown during mitosis, as well as exogenous retroviruses, which promotes entrance of LINE-1 into the nucleus.
It is worth noting that gene transcription is regulated by chromatin modifications, transcription factor regulation, and the rate of RNA degradation, while translational regulation of protein involves ribosome recruitment on the initiation codon, modulation of peptide elongation, termination of protein synthesis, or ribosome biogenesis. These two processes are controlled by different mechanisms, and therefore they may not always show the same change patterns in response to external challenges.
The Pfizer EMA assessment report also showed that BNT162b2 distributes in the spleen (<1.1%), adrenal glands (<0.1%), as well as low and measurable radioactivity in the ovaries and testes (<0.1%). No data on placental transfer of BNT162b2 is available from Pfizer EMA assessment report.
Results showed that BNT162b2 mRNA readily enters Huh7 cells at a concentration (0.5 µg/mL) corresponding to 0.5% of the local injection site concentration, induce changes in LINE-1 gene and protein expression, and within 6 h, reverse transcription of BNT162b2 can be detected.
https://www.mdpi.com/1467-3045/44/3/73/htm
https://pubmed.ncbi.nlm.nih.gov/33958444/
Pfizer Vaccine Becomes DNA in Liver Cells. (In-vitro Swedish Study)
Hepatitis (IN CHILDREN)
Recently, there have been reports of children with a severe acute form of hepatitis in the UK, Europe, the USA, Israel, and Japan. No common environmental exposures have been found, and an infectious agent remains the most plausible cause. Hepatitis viruses A, B, C, D, and E have not been found in these patients, but 72% of children with severe acute hepatitis in the UK who were tested for an adenovirus had an adenovirus detected, and out of 18 subtyped cases in the UK, all were identified as adenovirus 41F. However, adenovirus 41F has not previously been reported to cause severe acute hepatitis.
SARS-CoV-2 viral persistence in the gastrointestinal tract can lead to repeated release of viral proteins across the intestinal epithelium, giving rise to immune activation. Such repeated immune activation might be mediated by a superantigen motif within the SARS-CoV-2 spike protein that bears resemblance to Staphylococcal enterotoxin B, triggering broad and non-specific T-cell activation. This superantigen-mediated immune-cell activation has been proposed as a causal mechanism of multisystem inflammatory syndrome (MIS-C) in children.
Acute hepatitis has been reported in children with multisystem inflammatory syndrome, but co-infection of other viruses was not investigated. We hypothesize the recently reported cases of severe acute hepatitis in children could be a consequence of adenovirus infection with intestinal trophism in children previously infected by SARS-CoV-2 and carrying viral reservoirs.
In mice, adenovirus infection sensitizes to subsequent Staphylococcal-enterotoxin-B-mediated toxic shock, leading to liver failure and death. This outcome was explained by adenovirus-induced type-1 immune skewing, which, upon subsequent Staphylococcal enterotoxin B administration, led to excessive IFN-γ production and IFN-γ-mediated apoptosis of hepatocytes (liver cells).
Suggestion is that children with acute hepatitis be investigated for SARS-CoV-2 persistence in stool, T-cell receptor skewing, and IFN-γ upregulation, because this could provide evidence of a SARS-CoV-2 superantigen mechanism in an adenovirus-41F-sensitized host. If evidence of superantigen-mediated immune activation (i.e. ADE) is found, immunomodulatory therapies should be considered in children with severe acute hepatitis.
https://www.sciencedirect.com/science/article/pii/S2468125322001662
COVID19 vaccination can elicit a distinct T cell-dominant immune-mediated hepatitis with a unique pathomechanism associated with vaccination induced antigen-specific tissue-resident immunity requiring systemic immunosuppression.
https://www.sciencedirect.com/science/article/pii/S0168827822002343
Spike Protein and Mysterious Hepatitis in Children (Research Hypothesis)
Vaccine Spike induced T-Cell Myocarditis
In a cohort study of 23.1 million residents across 4 Nordic countries, risk of myocarditis after the first and second doses of SARS-CoV-2 mRNA vaccines was highest in young males aged 16 to 24 years after the second dose. For young males receiving 2 doses of the same vaccine, data were compatible with between 4 and 7 excess events in [only the first] 28 days per 100 000 vaccinees after second-dose BNT162b2, and between 9 and 28 per 100 000 vaccinees after second-dose mRNA-1273.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2791253
Clinical markers of T-Cell cardiac infiltration and damage have been shown to numerically increase and raise PULS scores from 11% to 25% for 5-year risk of Acute Coronary Syndrome (ACS) in a clinical setting of post-vaccinated patients. 11% to 25% is more than 100% increased risk after vaccination.
https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.10712
The S protein may elicit vascular cell dysfunction through CD147, independently from the infection. A recombinant S protein alone elicits cellular signaling through the CD147 receptor in cardiac pericytes, thereby inducing cell dysfunction and microvascular disruption.
Soluble S protein can potentially propagate damage to organs distant from sites of infection, promoting microvascular injury. Blocking the CD147 receptor in patients may help protect the vasculature not only from infection, but also from the collateral damage caused by the S protein.
SARS-COV-2 Spike Damages Heart Tissue and Vessels (IN-VITRO Study from UK)
Vaccine Spike Immunogen in Plasma
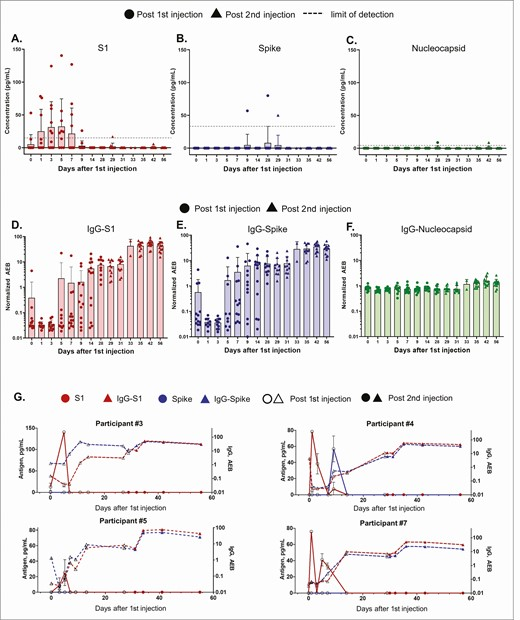
SARS-CoV-2 proteins were measured in longitudinal plasma samples collected from participants who received two doses of mRNA-1273 vaccine. 84% of Participants showed detectable levels of S1 spike protein as early as day 1 after first vaccine injection. Clearance of detectable SARS-CoV-2 protein correlated with production of immunoglobulin G (IgG) and immunoglobulin A (IgA).
https://academic.oup.com/cid/article/74/4/715/6279075?login=false
Spike Mediated Pericyte Dysfunction
ACE2 expression in human brain vascular pericytes was increased upon S protein exposure. Pericytes exposed to S protein underwent profound phenotypic changes associated with an elongated and contracted morphology accompanied with an enhanced expression of contractile and myofibrogenic proteins, such as α-smooth muscle actin (α-SMA), fibronectin, collagen I, and neurogenic locus notch homolog protein-3 (NOTCH3); Is this Ceroid Lipofuscin?
On the functional level, S protein exposure promoted the acquisition of calcium (Ca2+) signature of contractile ensheathing pericytes characterized by highly regular oscillatory Ca2+ fluctuations. Furthermore, S protein induced lipid peroxidation, oxidative and nitrosative stress in pericytes as well as triggered an immune reaction translated by activation of nuclear factor-kappa-B (NF-κB) signaling pathway, which was potentiated by hypoxia, a condition associated with vascular comorbidities that exacerbate COVID-19 pathogenesis. S protein exposure combined to hypoxia enhanced the production of pro-inflammatory cytokines involved in immune cell activation and trafficking, namely macrophage migration inhibitory factor (MIF).
Collectively, these findings suggest that SARS-CoV-2 S protein impairs the vascular and immune regulatory functions of brain pericytes, which may account for vascular-mediated brain damage.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8590447/
Vaccine Related Neurological Reactions
Various peripheral neuropathies, particularly those with sensory and autonomic dysfunction may occur during or shortly after acute COVID-19 illnesses. These appear most likely to reflect immune dysregulation. Observational studies suggest that a variety of neuropathic symptoms may manifest after SARS-CoV-2 vaccinations and in some patients might be an immune-mediated (ADE) process.
https://www.medrxiv.org/content/10.1101/2022.05.16.22274439v1
First Ever NIH/NIND Study on Vaccine Caused Neurological Injuries (Preprint)
Prion-Like Spike Protein
Prion diseases are a collection of neurodegenerative diseases that are induced through the misfolding of important bodily proteins, which form toxic oligomers that eventually precipitate out as fibrils causing widespread damage to neurons. The CDC website on prion diseases states that “prion diseases are usually rapidly progressive and always fatal.” It is now believed that many neurodegenerative diseases, including Alzheimer’s, Parkinson’s disease, and amyotrophic lateral sclerosis (ALS) may be prion diseases, and researchers have identified specific proteinaceous infectious particles linked to these diseases (Weickenmeier et al., 2019).
Prion proteins become toxic when the α-helices misfold as β-sheets, and the protein is then impaired in its ability to enter the membrane (Prusiner, 1982). Glycines within the glycine zipper transmembrane motifs in the amyloid-β precursor protein (APP) play a central role in the misfolding of amyloid- β linked to Alzheimer’s disease (Decock et al., 2016). APP contains a total of four GxxxG motifs.
When considering that the SARS-CoV-2 spike protein is a transmembrane protein, and that it contains five GxxxG motifs in its sequence, it becomes extremely plausible that it could behave as a prion. A paper published by J. Bart Classen (2021) proposed that the spike protein in the mRNA vaccines could cause prion-like diseases, in part through its ability to bind to many known proteins and induce their misfolding into potential prions. Idrees and Kumar (2021) have proposed that the spike protein’s S1 component is prone to act as a functional amyloid and form toxic aggregates. These authors wrote that S1 has the ability “to form amyloid and toxic aggregates that can act as seeds to aggregate many of the misfolded brain proteins and can ultimately lead to neurodegeneration.” According to Tetz and Tetz (2020), the form of the spike protein in SARS-CoV-2 has prion regions that are not present in the spike proteins for other coronaviruses.
Parkinson’s disease is a neurodegenerative disease associated with Lewy body deposits in the brain, and the main protein found in these Lewy bodies is α-synuclein. There are many parallels between α-synuclein and the spike protein, suggesting the possibility of prion-like disease following vaccination. We have already shown that the mRNA in the vaccine ends up in high concentrations in the liver and spleen, two organs that are well connected to the vagus nerve. The cationic lipids in the vaccine create an acidic pH conducive to misfolding, and they also induce a strong inflammatory response, another predisposing condition.
Germinal centers are structures within the spleen and other secondary lymphoid organs where follicular dendritic cells (innate immune system) present antigens to B cells, which in turn perfect their antibody response. Researchers have shown that mRNA vaccines, in contrast with recombinant protein vaccines, elicit a robust development of neutralizing antibodies at these germinal centers in the spleen (Lederer et al., 2020). However, this also means that mRNA vaccines induce an ideal situation for prion formation from the spike protein, and its transport via exosomes along the vagus nerve to the brain.
Studies have shown that prion spread from one animal to another first appears in the lymphoid tissues, particularly the spleen. Differentiated follicular dendritic cells are central to the process, as they accumulate misfolded prion proteins (Al-Dybiat et al., 2019). An inflammatory response upregulates synthesis of α-synuclein in these dendritic cells, increasing the risk of prion formation. Prions that accumulate in the cytoplasm are packaged up into lipid bodies that are released as exosomes (Liu et al., 2017). These exosomes eventually travel to the brain, causing disease.
https://www.mdpi.com/2076-2607/10/2/280/htm
A prion is a type of protein that can trigger normal proteins in the brain to fold abnormally. Prion diseases can affect both humans and animals and are sometimes spread to humans by infected meat products. The most common form of prion disease that affects humans is Creutzfeldt-Jakob disease (CJD).
https://www.hopkinsmedicine.org/health/conditions-and-diseases/prion-diseases
The number of Creutzfeldt-Jacob Disease (CJD)/prion disease reports in VAERS since the deployment of the COVID-19 injections has far surpassed the background rate for the U.S. for the year. Prion proteins or cellular prion proteins (PrPc), are native to humans, are in our brains, and expressed all the time. When these particular proteins mis-fold, then, Houston, we have a problem. These mis-folded proteins are called prions (mis-folded prion protein (PrPSc – Sc is for Scrapie2 3)) and are associated with neuro-degenerative diseases like Alzheimer’s disease. It seems that they can transform or ‘teach’ other prion proteins to mis-fold (transmissible), as well. It’s not really teaching as much as proximal disallowance of proper folding. This ‘enables’ an autocatalytic reaction whereby the PrPSc catalyzes the mis-folding of PrPc to produce more PrPSc due to the fact that prions are resistant to proteolysis – the process of ‘removal’ of mis-folded proteins.
https://jessicar.substack.com/p/rsfiedllfnkv-are-we-looking-at-weaponized?s=r
S1 Spike Protein meets the definition of a prion:
- S1 when binding to ACE2 causes inflammation, down regulates ACE2 formation, and ACE2 expression on the cell surface, thus upregulating ACE1.
- a7 nAChR may also be activated. If AChEsterase concentration exceeds cmc then Phospholipase concentration may “misfold” the phospho-lipid bilayer cell membrane.
- If MSH3 PRRA interacts with MSH2 at the site of neural genetic repair, or begins generating amyloid ceroid lipofuscin a la hermansky-pudlak syndrome sui generis in the brain misfolding platelets in an observed fibrinogenic characterized response, then S1 is a prion.
- If cytokine concentration from pyroptosis occurs in the microglia of the nervous system and degrades the myelin sheath, thus leading to a “misfolding” of neurons, then S1 is a prion.
- Research has also shown a displacement of zinc ions from the protein structure when S1 binds to ACE2, which causes them to misfold. The Displaced Zinc may further displace zinc embedded in other protein structures leading to further misfolding of proteins.
Long Covid & The Vagus Nerve
Findings point at vagus nerve dysfunction as a central pathophysiological feature of long COVID. Some of the most common symptoms of long COVID include fatigue, headaches, shortness of breath, loss of smell and taste, and muscle weakness. In a pilot evaluation, most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically-relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” Findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.
https://www.jpost.com/health-and-wellness/article-696452
N-Terminal Domain Toxicity
Zebrafish injected with fragment 16 to 165 (rSpike), which corresponds to the N-terminal portion of the protein, presented mortalities and adverse effects on liver, kidney, ovary and brain tissues. The conserved genetic homology between zebrafish and humans might be one of the reasons for the intense toxic effects followed inflammatory reaction from the immune system of zebrafish to rSpike which provoked damage to organs in a similar pattern as happen in severe cases of COVID-19 in humans, and, resulted in 78.6% of survival rate in female adults during the first seven days. The application of spike protein in zebrafish was highly toxic that is suitable for future studies to gather valuable information about ecotoxicological impacts, as well as vaccine responses and therapeutic approaches in human medicine.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8688160/
Lipid-NanoParticles
Lipid nanoparticles are next generation liposomes that use nanotechnology and are well suited to stable and efficient delivery of various therapeutics. Liposomes are closed lipid bilayer vesicles that spontaneously form in water (see fig. 1A) – essentially a fatty capsule. They were discovered in the 1960s and their potential as effective drug delivery systems was almost immediately recognized.
Liposomes have proven to be an extremely versatile nanocarrier platform because they can transport either hydrophilic drugs within the enclosed aqueous interior, or hydrophobic drugs within the hydrocarbon chain region of the lipid bilayer
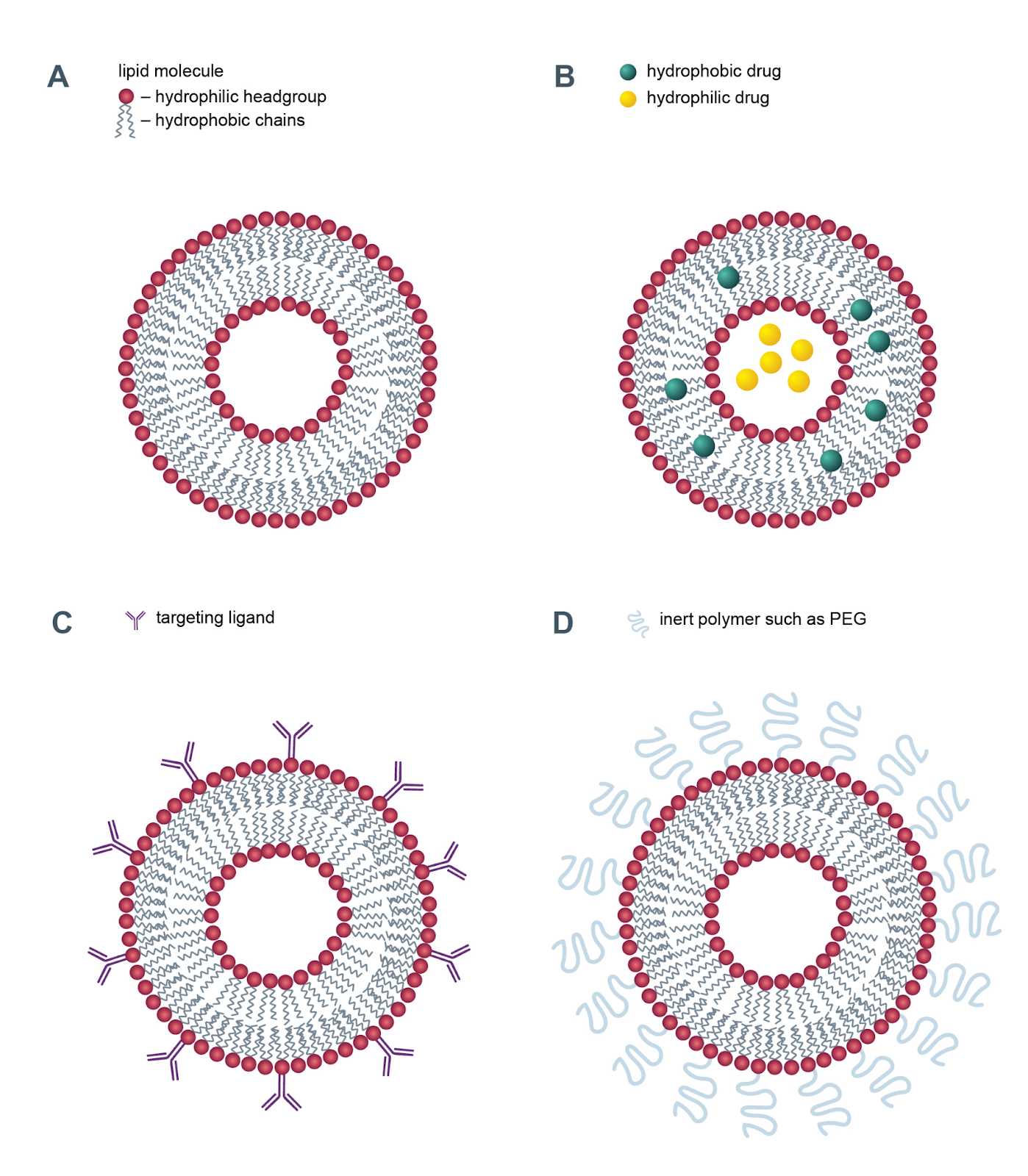
To enhance tissue targeting, the liposomes’ surface may be modified with ligands or antibodies which allow the liposome to recognise and bind to specific receptors on the cells. These are referred to as immunoliposomes.
To improve longevity in the blood stream, the surface may be coated in biocompatible inert polymers such as PEG, which goes undetected, like in the current Covid mRNA vaccines.
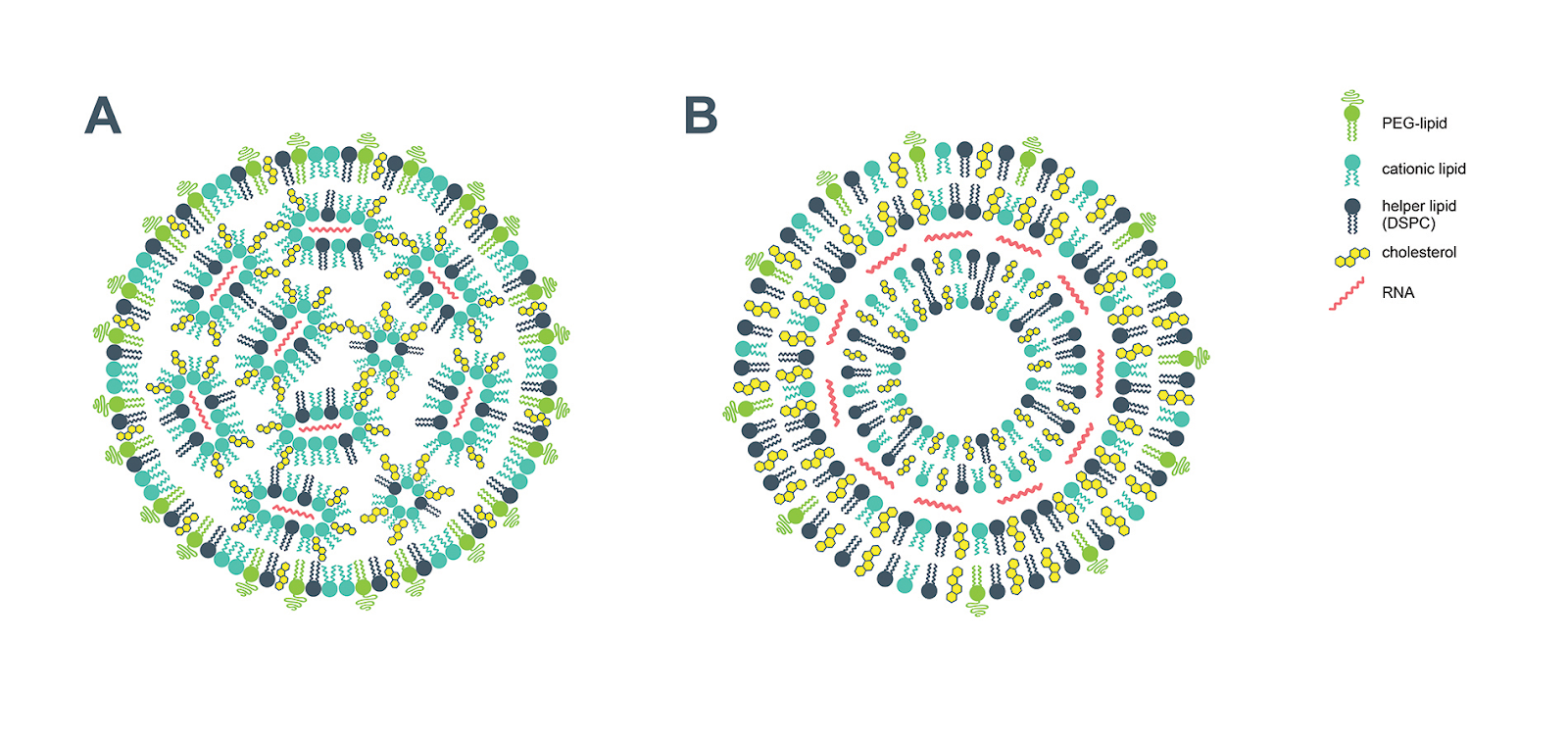
Presently, the most widely used non-viral vector system includes a synthetic positively charged (cationic) lipid. These form stable complexes known as lipoplexes with negatively charged (anionic) nucleic acids. Decorated by positively charged lipids, nucleic acids are more stable and resistant to nuclease degradation.
Despite their clear advantages for drug delivery, lipid nanoparticles have an unwanted side-effect; they have the potential to induce an allergic reaction, particularly for those who suffer with severe allergies. Researchers estimate a rate of 1.1 cases of anaphylaxis for every million first doses of the Pfizer/BioNTech COVID-19 vaccine. https://www.cas.org/resource/blog/understanding-nanotechnology-covid-19-vaccines
LNPs used in many preclinical studies are highly inflammatory in mice. Intradermal injection of these LNPs led to rapid and robust inflammatory responses, characterized by massive neutrophil infiltration, activation of diverse inflammatory pathways, and production of various inflammatory cytokines and chemokines. The same dose of LNP delivered intranasally led to similar inflammatory responses in the lung and resulted in a high mortality rate.
The intradermal inoculation of LNPs in mice led to the secretion of large amounts of major and minor pyrogens, IL-1β/IL-6 and macrophage inflammatory protein-α (CCL3) and macrophage inflammatory protein-β (CCL4), respectively (Figures 2B and 2C). Furthermore, the observed activation of other inflammatory pathways and cell death could further accentuate the experienced side effects. However, further studies will be needed to determine the exact nature of the inflammatory responses triggered by mRNA-LNP vaccines in humans and how much overlap there might be with the inflammatory signatures documented here for mice.
https://pubmed.ncbi.nlm.nih.gov/34938983/
Pharmacokinetics & Pharmacodistribution
Initially, 21 male rats were dosed at 100 ug mRNA/animal. Some adverse clinical signs were observed after approximately 24 hours post-dose and a subsequent review of the data showed concentrations were well detected in tissues. After discussions with the Sponsor, the target dose level was lowered to 50 ug mRNA/animal by amendment for the remainder of the study.
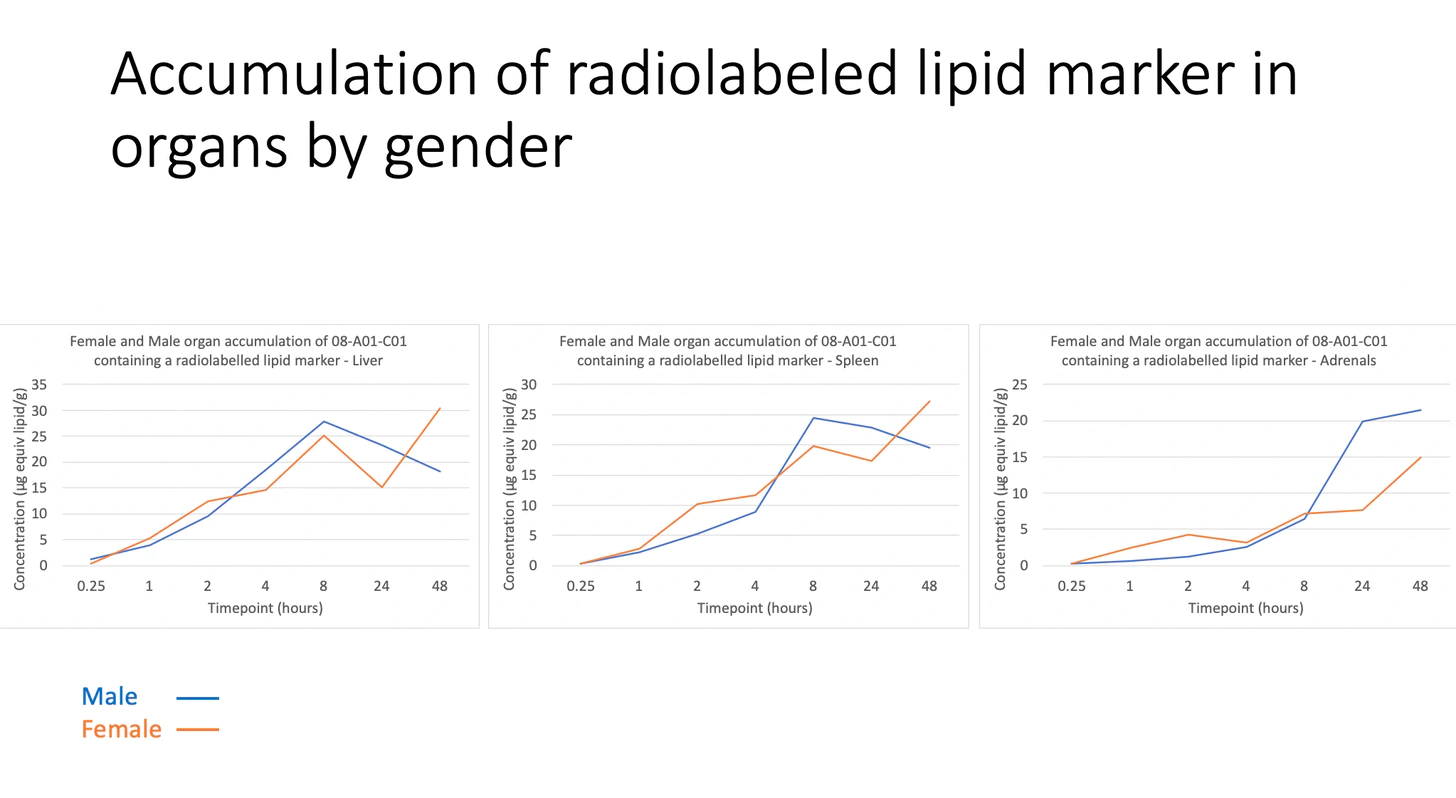
18.05% of the 50 ug dose accumulates in the liver after just 8 hours and remains at this concentration up to the 48-hour mark. It is unknown if this plateau trend continued or if the increase in percentage injected amount continued. The target dose level is 50 ug mRNA per animal with 1.29 mg total lipid per animal. So this means that the liver cells that contained the lipids had accumulations of 9 ug of mRNA and 0.23 mg of total lipid after just 8 hours.
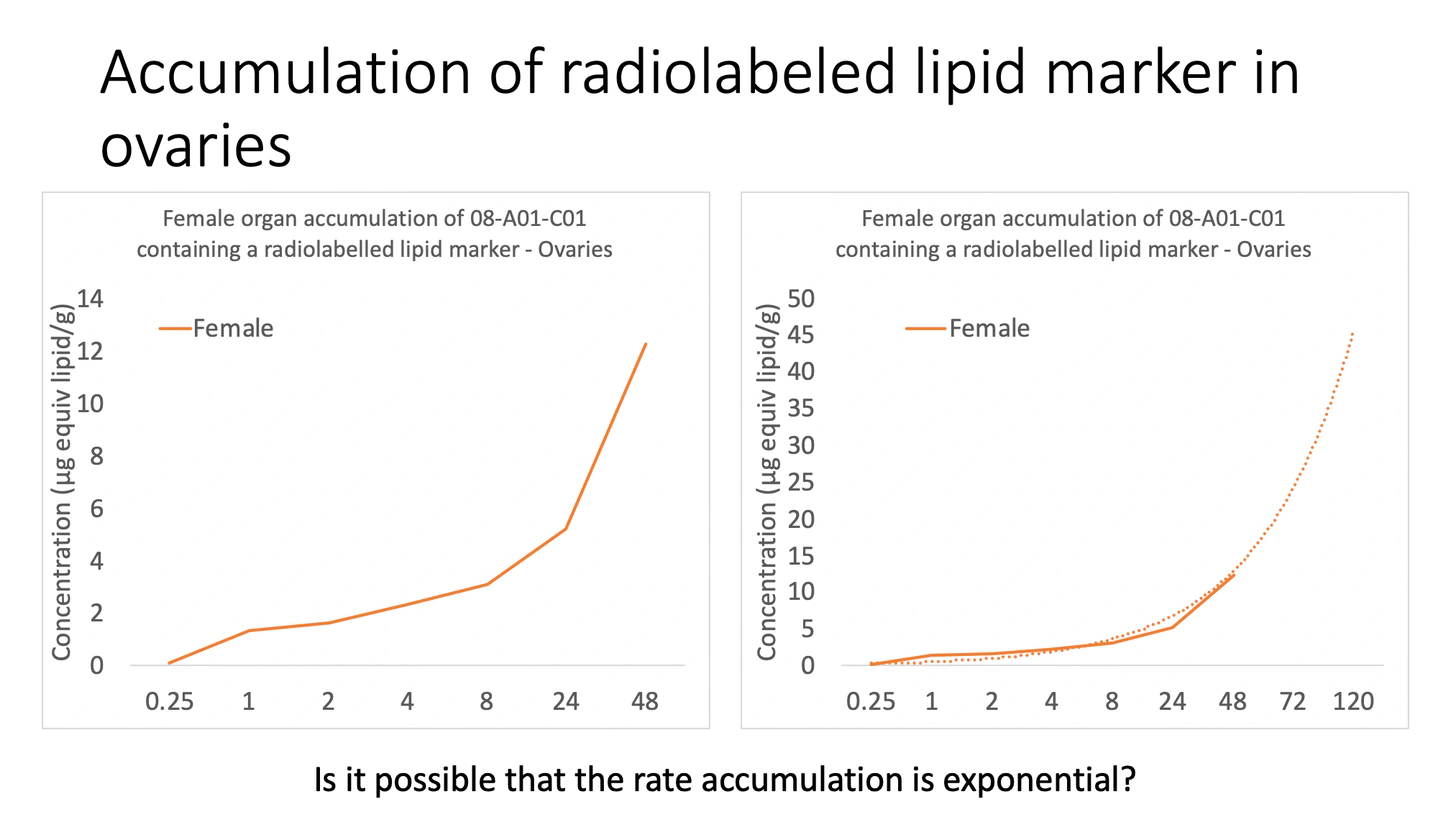
Although greatest mean tissue concentration remained at the injection site, biodistribution was clearly demonstrated and lipids were found in high concentrations in the liver, spleen, adrenals and ovaries following a short time period of 48 hours. Whether or not the accumulation continued following this time period is unknown.
https://jessicar.substack.com/p/the-pfizer-document-dump-pertaining?s=r
Reproductive
The European Medicines Agency’s safety committee reviewed reports of heavy menstrual bleeding and absence of menstruation from women who had received COVID vaccines from Pfizer/BioNTech and Moderna.
After reviewing the available evidence, the EMA’s Pharmacovigilance Risk Assessment Committee (PRAC) said it decided to request an evaluation of all available data, including reports from patients and healthcare professionals, clinical trials and the published literature.
Over more than 100 years, fewer than 40 cases of decidual cast shedding — during which the uterus’ thick mucous lining is shed, intact — have been reported. But over a 7.5 month period in 2021, 292 women experienced it, raising questions about whether Covid-19 vaccines could be to blame.
IVF clinics started having problems starting in March. And they’ve talked to other IVF clinics who are having similar problems:
- In March thru May, there was a huge spike in miscarriage rates. It is normally 25% to 30%. In these months it shot up over 50%. They’ve never seen anything like that before.
- One woman had very reliably donated 30 or more eggs each time she came in which yielded 5 to 8 embryos. In May, she got her second shot of the vaccine and then came in to donate a couple of weeks later. The clinic was shocked: all of the embryos had all arrested when they checked them on day 5. None of them reached the stage where the trophectoderm forms. I’m told this sort of thing is exactly what you’d expect from the vaccine (see “What happened in Singapore” below).
- They are seeing an unknown contaminant in the wells with the embryos. They started noticing this in August, but it could have started sooner than that. They only notice it under high power magnification and it is only the wells with the embryos. They still don’t know what it is or how it got there. Multiple clinics report the exact same thing. This means it is either coming from the sperm or the egg.
In one month, 2 of 10 women in their clinic are having serious problems. They both had 38 eggs but produced only 1 or 2 embryos, way below normal.
Various testicular cells including Leydig, Sertoli, spermatogonia and spermatozoa express ACE2 and related proteases resulting with viral fusion. Cytokine storm-induced dysfunction, autophagy regulation and damaged blood-testis barrier were also suggested as possible pathogenic mechanism for testicular damage. Clinical reports of orchitis, supported by histological findings, further emphasized testicular involvement. Detrimental impact on both spermatogenesis and testosterone production seem an obvious outcome; they evaluated donors from 3 sperm banks over a longitudinal period commencing before pfizer vaccine and following up after.
Post day 150, sperm concentration was -15.9% vs baseline, lower even than in the 75-120 day period. Average time post vaxx for T3 collection was 174 +/- 26.8 days so we’re talking about 6 months post vaxx with NO recovery in sperm concentration. Total motile count was slightly recovered from T2, but was still down 19.4% vs baseline, seeming to make up somewhat in volume what is lost in concentration. Both results were statistically significant at a 95% confidence interval and nearly so even at T3.
https://boriquagato.substack.com/p/pfizer-vaccine-effects-on-total-motile
Innate Immune Suppression
The BNT162b2 vaccine modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and non-specific (viral, fungal and bacterial) stimuli. The response of innate immune cells to TLR4 and TLR7/8 ligands was lower after BNT162b2 vaccination, while fungi-induced cytokine responses were stronger. In conclusion, the mRNA BNT162b2 vaccine induces complex functional reprogramming of innate immune responses, which should be considered in the development and use of this new class of vaccines.
https://www.medrxiv.org/content/10.1101/2021.05.03.21256520v1
Innate Immune System Reprogramming By Pfizer-BioNTech Vaccine Against SARS-COV-2?
Vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites.
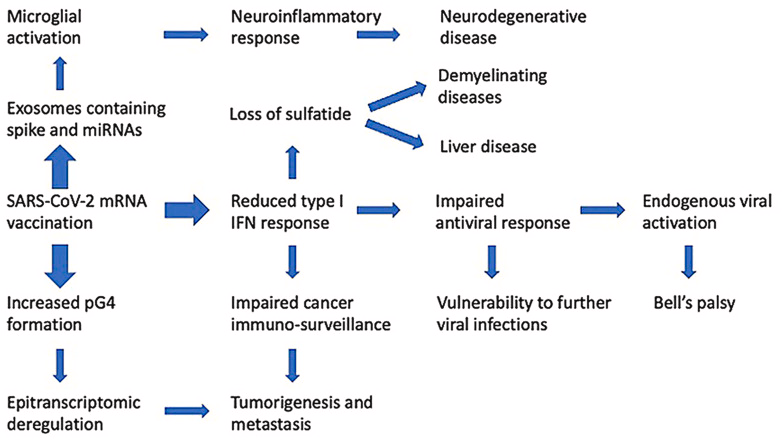
Seneff, et al also identified potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances potentially have a causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9012513/
This innate immune suppression is combined with immune system priming and may lead to antibody dependent enhancement of future pathogens infiltrating CD16+ or other primed macrophages upon natural infection or reexposure. Anti-Idiotype antibodies have been observed as a result of vaccination as well.
Child Vaccine Negative All-Cause Efficacy
Top epidemiologist Professor John Ioannidis has published a new study which concludes that the survival rate of people under the age of 20 who catch COVID is 99.9987%.
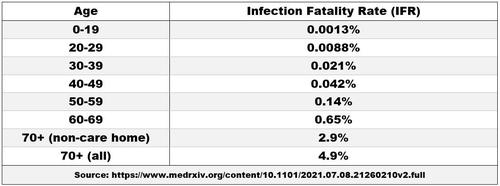
“From analysis of 25 seroprevalence surveys across 14 countries, Prof. Ioannidis and his colleague found the IFR varied from 0.0013% in the under-20s (around one in 100,000) to 0.65% in those in their 60s,” writes Will Jones.
The mRNA COVID vaccines begin a process of spike protein production throughout the body. Spike protein effects on ACE 2 receptors in the vascular endothelium serve to vasoconstrict. The result may obstruct the body’s supply of increased blood flow and oxygen, just when the demands are greatest, during exertion. Spike protein associated immune and inflammatory factors can also affect perivascular and periarterial cells, as well as CD8 and NK T-cell infiltration. All of these can reduce coronary vasodilation.
Further compounding the problem of blood delivery to peripheral and coronary tissues are the spike protein positions and effects. Jutting from the endothelial surface, spike proteins are docked onto ACE-2 receptors. These are thought to adversely affect blood flow through turbulent rather than laminar flow. As stagnant blood pools, the clotting cascade begins ubiquitously throughout the body. Such micro-clotting thickens and slows the blood, which would further impair the delivery of blood and oxygen to the capillary beds in the heart and in the periphery. Thus, coronary blood flow can be adversely affected by high viscosity, which is also caused by spike protein induced RBC aggregation from adhesion through CD 147. As a result, the heart is burdened to push a more viscous liquid than normal blood through the body’s arterioles and capillaries. Does this explain recent youth and athlete Sudden Death?
https://colleenhuber.substack.com/p/vaccinated-athletes-perform-worse?s=r
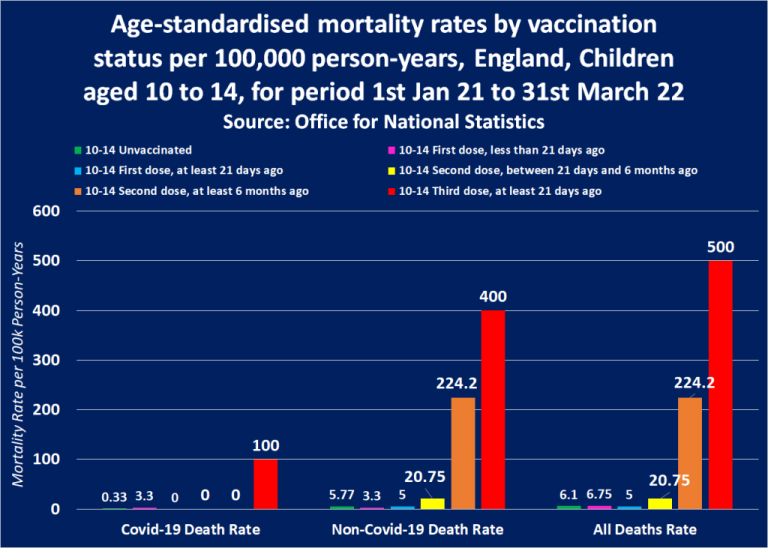
The Office for National Statistics has revealed without meaning to that children are 82 to 303x more likely to die following Covid-19 vaccination than children who have not had the Covid-19 vaccine.
There have also been reports of vaccine efficacy for children being 12% for 28 days. Combined with clinically observed ONS data, and the 99.9987% innate immunity, what is the medical justification to inject healthy children with this experimental gene therapy to produce the known biologic toxin as well as the inflammatory lipid-nanoparticles???
Results indicate that while T cells play a role in the recovery of rhesus macaques from acute SARS-CoV-2 infections, their depletion does not induce severe disease, and T cells do not account for the natural resistance of rhesus macaques to severe COVID-19. Neither primed CD4+ nor CD8+ T cells appeared critical for immunoglobulin class switching, the development of immunological memory, or protection from a second infection.
https://journals.asm.org/doi/10.1128/mBio.01503-21
What reason is there to artificially induce the creation of CD8+ Tcells in children with “boosters” when Alpha strain B.1.1.7 is no longer in natural circulation?
Boosters May Weaken The Immune System Says European Medicine Agency (EMA) | T Cell Exhaustion
A Lancet study comparing vaccinated and unvaccinated people in Sweden was conducted among 1.6 million individuals over nine months. It showed that protection against symptomatic COVID-19 declined with time, such that by six months, some of the more vulnerable vaccinated groups were at greater risk than their unvaccinated peers.
Doctors are calling this phenomena in the repeatedly vaccinated “immune erosion” or “acquired immune deficiency”, accounting for elevated incidence of myocarditis and other post-vaccine illnesses that either affect them more rapidly, resulting in death, or more slowly, resulting in chronic illness.
Using national epidemiological and whole genome sequencing surveillance data from March to August 2021 in the Netherlands, our analysis provides evidence for an increased risk of infection by the Beta, Gamma, or Delta variants compared to the Alpha variant after full vaccination, regardless of the vaccine used. This indicates lower vaccine effectiveness against infection with the Beta, Gamma and Delta variant compared to the Alpha variant. No clear differences between vaccine type were observed as confidence intervals largely overlap.
https://www.medrxiv.org/content/10.1101/2021.11.24.21266735v1
Children under 18 are also 51 times more likely to die from the jab than they are to die from COVID if not vaccinated.
https://www.theepochtimes.com/the-alarming-trends-in-covid-jab-side-effects_4319841.html
https://www.naturalnews.com/2021-11-19-covid-vaccines-suppressed-immunity-hiv-hpv-herpes.html#
Th1-Th2 Pathways & CD8 Concentration
CD4+ cells are the earliest state of existence any adaptive antibody can be. All antibodies originate as CD4+ T-helper (Th) cells.
CD4+ cells of the adaptive arm of the immune system may turn into Th1 or Th2 cells:
- Th1 cells turn into CD8+ Killer T-Cells.
- Th2 cells turn into B-memory cells.
Fauci, WHO, CDC, and the medical establishment have sold the world on the idea that CD8+ cytotoxic killer T-cell antibodies must be present at a specific concentration, in order for “immunity” to exist within the body.
To solely rely on a quantitative measure of the adaptive immune system, thinking an increase on the Th1 pathway to CD8+ cells is the ONLY way to treat a viral SARS/Airborne pandemic, completely discounts the efficacy of the innate immune system; An innate immune system upon which accounts for a 99.99% “natural immunity” in children, and is responsible for processing biological matter into the protein antigens needed to program CD4+ cells in the first place…
Public Health Gain of Function Research
Th2 immune pathology is based on a subset of CD4+ pathways the adaptive immune system may take regarding a vaccine or any other pathogen. “Th1 cells drive the type-1 pathway (“cellular immunity”) to fight viruses and other intracellular pathogens, eliminate cancerous cells, and stimulate delayed-type hypersensitivity (DTH) skin reactions. Th2 cells drive the type-2 pathway (“humoral immunity”) and up-regulate antibody production to fight extracellular organisms; type 2 dominance is credited with tolerance of xenografts and of the fetus during pregnancy.” https://pubmed.ncbi.nlm.nih.gov/12946237/
The Th2 humoral response is held in concert with Th1. Th2 immune pathology is science speak for when Th2 becomes dominant over Th1. Th1 is considered preferential in viral immunology, because the cellular immune response leads to the creation of CD8+, cytotoxic specialized killer T-cells. CD8+ cells are “antibodies” pharma companies use as the “gold standard” for proof of efficacy and continuing Emergency Use Authorizations…
In 2014 Evaluation of available SARS-based immune-therapeutic and prophylactic modalities revealed poor efficacy; both monoclonal antibody and vaccine approaches failed to neutralize and protect from infection with CoVs using the novel spike protein.
Doubly inactivated vaccines induced a Th2 immune pathology associated with massive influxes in the numbers of eosinophils and neutrophils, effectively causing a gain in virus pathogenic potential in an unpredictable manner (Bolles et al., 2012). The resulting increased immune pathology can sometimes progress to fatal disease and similar findings have been reported in primates.
https://www.nature.com/articles/nm.3985
Dr. Baric, of WIV, Wuhan, China fame, cited research that inducing T-Helper 2 (CD4+) cells associated with an increase in white blood cells effectively causes a “gain of virus pathogenic potential”. Baric, et al synthetically re-derived an infectious full-length SHC014 recombinant virus and demonstrated robust viral replication both in vitro and in vivo. The work suggested a potential risk of SARS-CoV re-emergence from viruses currently circulating in bat populations. When biological mechanisms involving the immune system make a virus WORSE it gave reason for a moratorium on pathogenic research in 2014.
Public Policy was forced to shift and create the Potential Pandemic Pathogens (PPPs) and was buffered by Cambridge Working Group Consensus Statement on the Creation of Potential Pandemic Pathogens (PPPs):
“For any experiment, the expected net benefits should outweigh the risks. Experiments involving the creation of potential pandemic pathogens should be curtailed until there has been a quantitative, objective and credible assessment of the risks, potential benefits, and opportunities for risk mitigation, as well as comparison against safer experimental approaches.”
http://www.cambridgeworkinggroup.org/documents/statement.pdf
This approach must be considered in the context of the US government–mandated pause on gain-of-function (GOF) studies. On the basis of previous models of emergence, the creation of chimeric viruses such as SHC014-MA15 was not expected to increase pathogenicity. Although SHC014-MA15 is attenuated relative to its parental mouse-adapted SARS-CoV, similar studies examining the pathogenicity of CoVs with the wild-type Urbani spike within the MA15 backbone showed no weight loss in mice and reduced viral replication. Thus, relative to the Urbani spike–MA15 CoV, SHC014-MA15 shows a gain in pathogenesis.
Gain in pathogenesis = Gain of Function. The moratorium on gain of function was tailored to reduce the amount of antibodies ultimately produced by the Th2 humoral response in order to limit the overproduction of non-neutralizing eosinophils and neutrophils which caused further damage. Today’s medical lexicon may call this action Antibody Dependent Enhancement.
Whatever term “gain of function” may have for public policy experts, the observable effects of an MSH3 gene, known to be associated with ceroid lipofuscin formation and bleeding disorders MUST be looked at closer. As well as, N-Terminal, ACE2 effects, a7 nAChR effects, lipid-nanoparticle effects, and spike protein sui pathogenesis in general.
Emerging viruses exist in swarms of heterologous but related viruses, thus, Future outbreaks could be derived from other precursor strains which are antigenically and genetically distinct. Antigenic variation could obviate the potency and efficacy of SARS vaccines and immunotherapeutics or erode the therapeutic potency of antiviral drugs.
Vaccines using the SARS S glycoprotein do not protect against lethal heterologous Spike challenge, Especially in aged animals; Thus, current SARS vaccines will fail to protect against these precursor strains should they seed future outbreaks. In fact, the doubly inactivated vaccines don’t protect but do stimulate the Th2 immune pathology noted above
“Gain-of-function” research produces the unwanted result of an increased pathogenic, non-neutralizing response within the immune system. Gain of function implies harm to the organism itself via an increased biological functioning, leading to greater or increased pathogenicity within the body or host. No scientist will admit conducting research leading to harm being done to people. If they did, they would in essence, be providing a function for a system antithetical to medical ethics. The creation of the PPP distinction insulated the scientific community by providing a whipping boy the erudite establishment could collectively scoff at and label “Gain-of-function” in disdain.
https://dockek.substack.com/p/they-knew-the-danger
Recall the antibody targets at the beginning of Part 3 for the current vaccines being B-Cells, i.e. Th2 response. The emerging variants of concern are precursor strains exposed to non-neutralizing antibodies. Many believe the “new” variants have evolved from SARS-CoV-2 Alpha B.1.1.7 strain, and that is NOT the case, as variants are categorized by changes in spike protein ONLY, and may NOT be related to SARS phylogenetically.
The schism of “gain of function” by the creation of the PPP label is what Dr. Fauci and other public policy experts hide behind, because no one else delineates pathogenic research, in all of its forms, from “gain of function”. However, there is little doubt continuing to inject a spike protein from a virus two years ago, no longer in natural circulation, will only go to forwarding the probability of a gain in pathogenesis in those continuing to be injected, to include children.
CD8+ concentration CANNOT be used as a measure for “immunity” because scientific research has shown elevated concentrations to be associated with a gain of function, or gain in pathogenesis of the antigen within the host’s body. The effects on the host’s body are unknown for chronic exposure. Informed Consent must be provided on each item contained herein to ensure proper medical disclosures are provided, and patients made fully aware of the cascade of effects, to include mutagenic influence on their own genome.
Many Blessings

Leave a comment